Any muscle that is tight in a baby’s neck has the potential to complicate breastfeeding. As an IBCLC, I work with mothers and babies to get a comfortable position and latch. Mothers contact me when this is proving difficult – for either them or their baby. Musculoskeletal issues in the baby is one reason for this difficulty. Muscles can be damaged during the birth or from restrictive inutero positioning. In order to breastfeed, mothers will resort to all sorts of intricate compensations and modifications, but ultimately, we need to address the root cause. As a craniosacral therapist I believe bodywork is crucial for these babies!1 Completely comfortable breastfeeding is often not possible until the issue resolves. In some cases, it may take months and mothers will then struggle to meet their breastfeeding goals. In this article I discuss the two most common neck muscle injuries that I treat in babies – the digastric muscle and the sternocleidomastoid muscle. I dissect the similarities and differences between these two key muscles, how breastfeeding is impacted and how to help these babies with breastfeeding.
Firstly, let me introduce you to the digastric muscle….
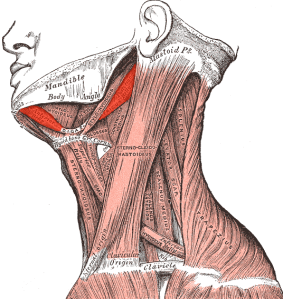
The digastric muscle (meaning two bellies) is, in my experience, an overlooked culprit that doesn’t appear to get any attention in regards to its importance in breastfeeding. This paired muscle is situated under both sides of the jaw and is involved in swallowing and opening the mouth. If it gets damaged you can imagine its negative impact on breastfeeding! In my craniosacral/lactation practice, I have been noticing this come up as the root cause of breastfeeding difficulties in quite a few babies over the last few months. I have been unable to find much info on it in relation to breastfeeding on the internet so wanted to share more about this injury and the importance of bodywork / CST in these babies. Often only one side and one “belly” is tight and most likely due to a birth injury.
It can be damaged during a c-section – if the surgeon had difficulty removing the baby from the uterus and unintentionally grips too tight around the jaw/under the chin. Similarly with vaginal births. One baby client of mine had had a very tightly wound umbilical cord around their neck and the digastric muscle was injured in the process of removing the cord. It can also be damaged by the use of misplaced forceps. Damage may occur to the muscle itself or to one of the cranial nerves that innervate the muscle (more on this below).
See the placement of the birth attendants fingers in both these photos…


Signs/Symptoms/Impact on breastfeeding include:
- Difficulty swallowing – increased swallowing of air, choking, clicking, gassiness /reflux
- Asymmetrical lower jaw / mouth
- Poor latch – can’t open mouth wide to latch, needing to use a nipple shield
- Infant discomfort
- Fussy at breast
- Breast refusal
- Nipple pain
- Poor milk transfer
- Head turn preference or tilt (less obvious than torticollis)
- Breastfeeding is painful or more difficult on one side
What it may feel like to baby:
As far as the internet goes, we don’t seem to have recognised that this particular injury can be an issue for babies but adults who experience a digastric muscle injury report jaw, throat, tooth, and general facial pain. As an empath I can mirror a baby’s physical symptoms in my body during a cranio treatment and what I notice is pain or discomfort in one ear or under the jaw. This would be exacerbated by swallowing or opening the jaw. There can be general discomfort and mothers report babies are quite unsettled or a high needs baby.
Interestingly, the digastric muscle is innervated by two different nerves. The trigeminal nerve connects to the anterior belly and the facial nerve connects to the posterior belly. It is possible that injury to the nerve is the cause of the muscle tightness (rather than physical injury to the muscle as mentioned above)2. Both the facial nerve and the trigeminal nerve connect to different parts of the face, thus, any tension in either part of the muscle can send pain impulses through many parts of the face and jaw. I have noticed babies in treatment rubbing their faces or mums reporting that it appears like their baby is teething (in younger babies).
The digastric muscle attaches behind the ear, at the mastoid notch and works in a pulley-like fashion connecting to the chin via the hyoid bone – a free-floating bone under the chin. My experiences show that it tends to be the posterior belly of the digastric that is tight on one side. The tongue also attaches to the hyoid bone which is why any tension in the digastric muscle tends to affect swallowing and sucking. The paired digastric muscles help raise the hyoid bone during speech and swallowing and facilitate opening the mouth. In breastfeeding babies it is important to open the mouth wide to latch and for the coordination of the suck/swallow/breathe reflex3.
Because this muscle is not recognised as a cause of breastfeeding difficulties, mothers may be told their baby has torticollis, but typically, torticollis (meaning “wry neck”) involves the sternocleidomastoid muscle (SCM)4. The SCM is a well-known cause of breastfeeding difficulties. Torticollis does indeed, share some of the above signs and symptoms. The difference, I feel, is torticollis is more visibly obvious and tends to affect latch and getting a comfortable position at the breast as baby’s head is not in alignment with the rest of the body, whereas the digastric has more of an impact on ability to open the jaw wide and on swallowing and sucking. It may be less obvious.
More about torticollis and the SCM…
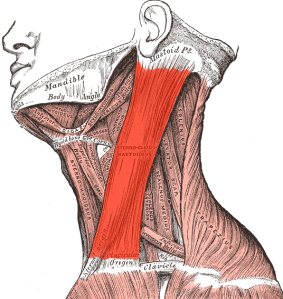
The SCM is also a paired muscle on each side of the neck. The SCM is a long muscle and connects the skull to the collar bones. In torticollis one of the SCM tends to be shorter or tighter and causes the head to tilt to one side and the head to turn to the other. Torticollis is more likely to be caused by restrictive inutero positioning or abnormal growth of the SCM on one side. Though the SCM, like the digastric muscle, can also be damaged during birth e.g. by forceps or a pulled muscle. Anatomically, both the SCM and the digastric muscle attach to the same place -temporal bone, an area called the mastoid notch behind the ear.
Signs and symptoms include:
- Difficulty latching – needing to use a nipple shield
- Infant discomfort
- Fussy at breast
- Breast refusal
- Nipple pain
- Poor milk transfer
- Head turn preference or tilt
- Breastfeeding is painful or more difficult on one side

In this photo you can see a “pseudo” SCM tumour. This little one was born with misplaced forceps. I treated her at the age of four as she had head pain while travelling in the car. I could feel this restriction still present in her system.
Photo shared with permission
This little one had an obvious head tilt prior to 3-4 sessions of CST to treat his torticollis.
Photo shared with persmission

In both these conditions, babies are in pain/discomfort and with torticollis it hurts to turn their head. Lactation consultants can assist mothers with positions that allow the baby to latch within the bounds of their comfortable head tilt or turn. Babies with asymmetry/head preference will not want to have their head centred so best not to force this. Some mothers have success with lying down when breastfeeding as the baby can be lying in their position of ease and the mother can accommodate. Another hold that might be useful is the koala hold, which is upright straddle feeding (some mothers may need to lie back to elongate their torso). Whether it is the digastric or SCM muscle that is causing the issue, the key is to work out which position is most comfortable for them and as much as possible offer the breast in this position.
The usual referral pathway within the health system for torticollis is to see a paediatric physiotherapist who will prescribe exercises /stretches and recommend positions to encourage baby to turn the head. The guppy pose or modified guppy may be helpful for babies with a tight digastric muscle:
As a bodyworker, I would encourage parents to look outside of the system for more help from complimentary therapies like craniosacral therapy. Craniosacral therapy is the gentlest of bodywork! It is non manipulative and works by facilitating a healing state in the baby and triggering the body’s own self-healing mechanism. It is a good idea to seek out bodywork early as the longer a baby holds these tensions and compensations, the longer it will take to heal4.
Mothers (of my baby clients who were found to have these type of injuries) have reported :
- better sleep
- improved feeding
- reduced reflux
- more settled behaviour
- improvement in head preference
If you feel your baby would benefit from cranio treatment. Get in touch with Jenny today.
Footnotes:
1.Often babies with musculoskeletal injuries get diagnosed with colic. A recent study shows 1-3 sessions of craniosacral therapy resolved colic symptoms. This study also showed an improvement in neck pain and function (and quality of life) in adults who received CST.
2.Facial palsy is caused by damage to this nerve.
3.Older children and adults also use this muscle to chew and speak.
4. Torticollis/head tilts may also have cranial nerve/ visual causes or related to bones of the vertebra.
5. Untreated torticollis can lead to issues with range of motion of the neck (long term), persistent cranialfacial asymmetry (e.g. plagiocephaly) and scoliosis. Babies with an untreated chin tilt, process their world on an angle which may then develop into ongoing issues with visual field development.
